

Introduction: Why Choosing the Right Cooking Oil for Diabetics Matters:
Choosing the right cooking Oil for people with diabetes matters more than most people realise.
For those with diabetes, oil is not merely a source of calories; Rather, it influences inflammation, insulin sensitivity, lipid profile, and long-term cardio metabolic risk.
Consequently, when deciding which oil to use for daily cooking, consider the fatty acid composition, stability during heating, antioxidant content, and clinical research evidence.

Commonly Used Oils:
In this article, we compare five commonly used oils: extra virgin oil, canola oil, avocado oil, sunflower oil, and coconut oil, and evaluate them for people living with diabetes. First, we review history and chemistry.
Next, we explain how ancient peoples managed oils for health. Then, we examine how oils affect diabetes through psychological mechanisms and clinical research.
Finally, we present a research-based verdict and practical selection guide.
How Ancient People Used Cooking Oil for Diabetics and Other Diseases:
Ancient healers used oils not only for cooking but also for treating ailments. For instance, olive oil appeared in Hypocrite Recipes & was applied topically or consumed with herbs to support digestion and “balance humours”.
An ayurvedic and traditional Pacific medicine, coconut oil serves both culinary and therapeutic roles, believed to aid digestion and promote healing.
Although ancient clinicians did not understand insulin or glycemia, they associated certain fats with society, body strength, and recovery.
Importantly, additional extraction methods (cold pressing, sun separation, fermentation) preserved many bioactive compounds, which likely contributed to observed health effects.
In short, the ancient people avoured minimally processed oils. A practice that modern science often supports for metabolic health.

Introductory Chemistry of Cooking Oils:
Oils are mixtures of triglycerides, with three fatty acids attached to a glycerol backbone. Fatty acids are classified as saturated (SFA).
Monounsaturated (MUFA) or polyunsaturated (PUFA). Each class influences metabolism differently:
- Saturated fat (no double bonds) tends to raise LDL cholesterol and may worsen cardio-metabolic risk when consumed in excess.
- Monounsaturated fats (MUFAs), such as oleic acid, generally improve insulin sensitivity and lipid profiles.
- Polyunsaturated Fats (PUFA): include linoleic acid (omega 6) and alpha linoleic acid (ALA omega 3). Many PAFUs support cardio metabolic health when they replace SFAs.
Beyond fatty acids, minor components such as polyphenols, tocopherols (Vitamin E), phytosterols, & other antioxidants protect oils from oxidation and can provide independent metabolic benefits. Extra virgin and cold-pressed oils usually retain more of these compounds than refined oils.
Fatty Acids and Property Comparison:
| Oil | Typical SFA % | MUFA% | PUFA% | Typical Smoke point(°C) | Notable minor Compounds |
| Extra virgin olive oil | ~10-20 | ~60-80 | ~5-15 | 160-190(EVOO varies) | Polyphenol, oleuropein, tocopherols. |
| Canola oil (refined) | ~7 | ~60-65 | ~25-30 | 200-240 | Some vitamin E, low saturated fat; modest ALA (omega-3) |
| Avocado oil | ~10-18 | ~60-75 | ~10-15 | 200-270 (refined) | Sterols, carotenoids, tocopherols; high MIFA. |
| Sunflower oil(common) | ~10 | ~20-25 | ~60-70 (linoleic) | 225-240 | Vitamin E; high linoleic acid in conventional varieties. |
| Coconut oil | ~80-92 | ~6 | ~1-2 | 175-200(refined) | MCFAs (lauric acid): low antioxidants unless virgin. |
Role of Cooking Oil for Diabetics in Managing Blood sugar and health:
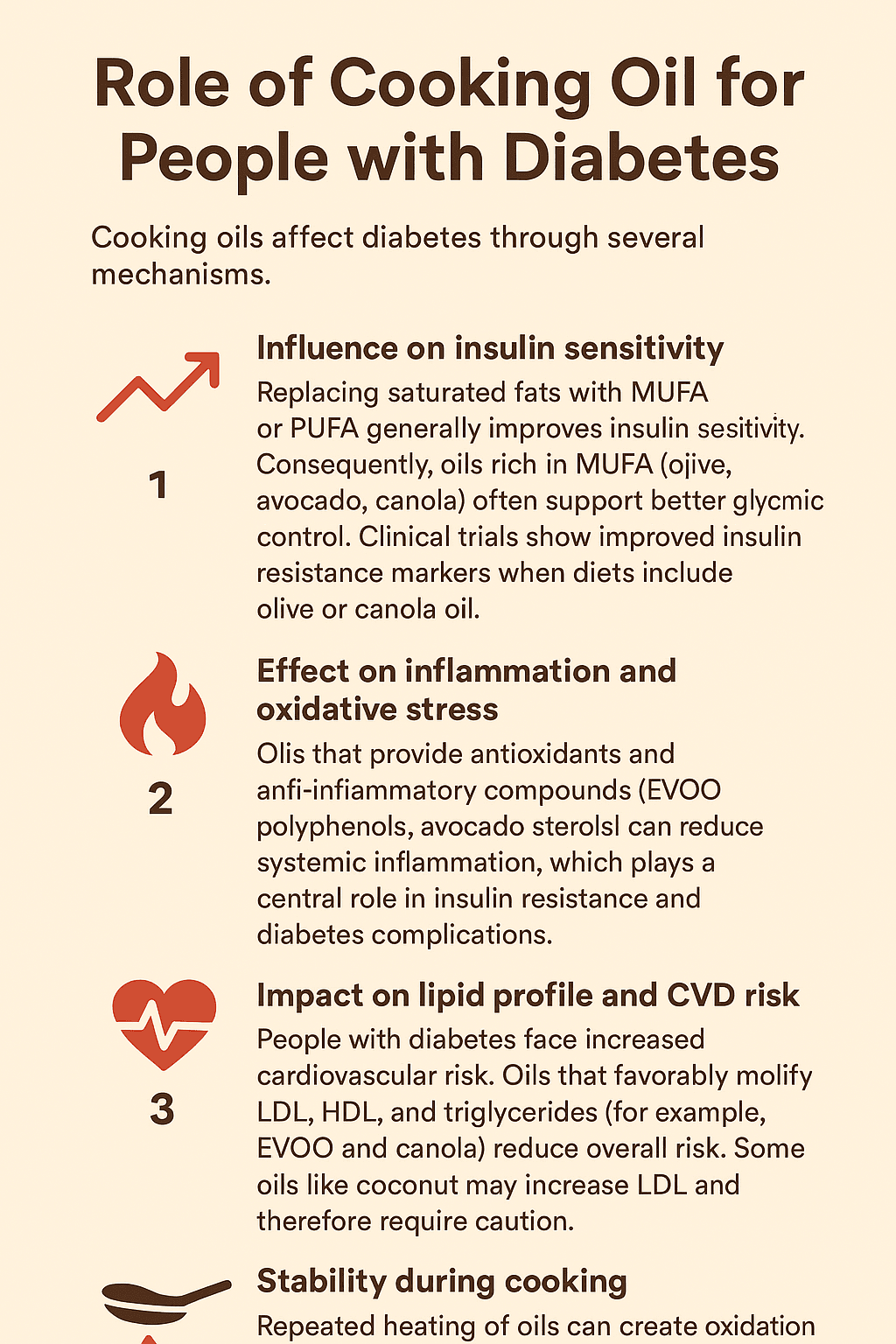
How Cooking Affects Diabetes Mechanisms: Explain:
To decide which oils are best, you must understand the mechanism:
- Membrane composition & insulin signalling: dietary fats incorporate into cell membranes & affect insulin receptor function. MUFAs & PUFAs tend to preserve membrane fluidity & promote signalling, while excessive SFAs can impair signalling pathways.
- Lip Toxicity: Accumulation of specific lipid species in the liver, muscle, and pancreatic beta cells contributes to insulin resistance. Replacing SFAs with MMUFs / PUFAs lowers harmful lipid intermediates.
- Inflammation: Some PUFAs (omega-3) & polyphenols are anti-inflammatory, whereas oxidation products from overheated oils promote inflammation. Therefore, antioxidant-rich oils and proper cooking practices reduce pro-inflammatory signals.
- Post Prandial glycaemia: Fats slow gastric emptying & blunt postprandial glucose spikes, but the quality of fat Long term metabolic responses oils that improve insulin sensitivity & help control both fasting and postprandial glucose.
Research-Based Data: Cooking Oil for Diabetics,
Three Studies, with the evidence.
1. Olive oil and diabetes risk dose-response meta-analysis:
Cooking Oil for Diabetics:
A recent dose-response meta-analysis found that olive oil consumption is associated with a Lower risk of type 2 diabetes, & consuming roughly 10-20 g/day correlated with a measurable benefit.
The Mediterranean diet trials that supplemented diets with EVOO demonstrated improved glycaemic control & lower incidence of metabolic syndrome; thus, EVOO has robust epidemiologic and trial support.

2. Canola Oil Improves Insulin Resistance Markers in Trials:
Cooking Oil for Diabetics:
Randomised clinical trials comparing canola & olive oils showed that replacing higher SFAs with canola or olive oil improved markers of insulin resistance, inflammation, and oxidative stress in adults with or at risk for type 2 diabetes.
These controlled feeding studies support the use of canola as a programmatic, affordable MUFA-rich option.

3. Avocado Oil Shows Promising Metabolic Benefits:
Human and animal studies indicate that avocado oil may enhance glycaemic control and lipid metabolism, likely due to its high MUFA content and beneficial phytochemicals.
However, evidence remains smaller in scale than for olive oil; therefore, avocado oil is promising but needs larger randomized trials.

4. Coconut Oil Mixed Signals and Lipid Concerns:
Coconut oil trials show mixed effects, with some short-term effects. Studies report improved HDL or subjective well-being, but systematic reviews and meta-analyses highlight increased LDL cholesterol and potential increases in insulin resistance with long-term consumption of saturated fats.
Hence, Coconut oil is controversial for diabetics and should be used cautiously.

5. Sunflower and Other Seeds Oil Context Matters:
Cooking Oil for Diabetics:
Seeds oil high in linoleic acid (a common form of sunflower oil) has been associated with improved heart disease outcomes in some epidemiologic studies.
While experimental modes show mixed effects on inflammation and insulin resistance depending on overall diet and omega-3 balance, importantly, high oleic sunflower oil (MUFA-rich) behaves more like olive/avocado oil and is preferable to high-linoleic varieties for some metabolic endpoints.

Modern Research Consensus and Interpretive Notes:
Overall, Modern research points in a clear direction:
Replace high SFA intakes with MUFAs/PUFA sources and favour oils with natural, handy acids. When possible, extra virgin Olive oil sits at the top of the evidence; Parliament for diabetes prevention and metabolic benefits. Canola and avocado oils provide important MUFAs & are practical alternatives.
Seeds Oils:
Seeds oils like sunflower can be either helpful or neutral depending on their fatty acid profile, whereas coconut oils’ high saturated fat content warrants caution.
Moreover, research consistently shows that oils are best evaluated within whole dietary patterns (for example, a Mediterranean Diet plus EVOO produces greater benefits than isolated oil supplementation).
Practical Comparison: Best and Worst Diabetics:
| Oil | Why | How to use | Evidence |
| Low SFA, high MUFA, some ALA: affordable and heat-stable. Helps improve insulin resistance when replacing saturated fats. | Use for salad, dressings, light cooking; avoid deep frying. | Meta-analysis and trials confirm improved glycaemic control | Extra virgin olive oil: Best choice overall |
| Good for roasting, dressings & medium-high heat cooking | Refined canola for frying cold cold-pressed for daily use. | Canola oil: Very good option | Controlled trials show better liver fat & insulin response. |
| Avocado oil Heart-friendly | Very high MUFA: contains sterols & carotenoids. Early studies suggest glycaemic & lipid benefits | Sunflower oil mixed prefers high-oleic | Small studies show positive metabolic outcomes. |
| Choose high oleic for cooking, limit standard type unless balanced with omega-3 | Regular sunflower has high omega-6; excess may raise inflammation. High oleic type behaves like olive oil. | Sunflower oil Mixed prefers high-oleic | Mixed evidence; omega-6 effects depend on diet balance. |
Coconut Oil use with Caution (Worst of the five for many people with diabetes):
- Why: Very high saturated, fat content, short-term studies report mixed effects, but meta-analysis raises concerns about LDL increases and limited benefits for long-term glycaemic control.
- How to use: Use sparingly: Consider virgin coconut oil for flavour in small amounts, but do not rely on it as a primary oil for diabetics.
- Evidence: Systematic reviews indicate coconut oil can raise LDL; other studies find transient benefits, but not sustained glycaemic improvement. Therefore, coconut oil is not a first-line choice for people with diabetes.
At Least Three Research Data Points Summarized:
- Dose response for olive oil: A meta-analysis found that daily olive oil intake of 10-20 grams is linked to reduced diabetes risk. This finding supports the inclusion of EVOO as a primary fat source in metabolic health plans.
- Canola vs saturated fats: Randomised feeding trials show that replacing saturated fats with canola oil improves insulin resistance markers and reduces liver fat indices in at-risk adults. This demonstrates the metabolic advantage of lowering SFA intake.
- Avocado oil benefits. Human supplementation studies on avocado oil’s effects on fasting and insulin levels and lipid markers require larger-scale RCTs to confirm its impact across varied populations.
Practical tips for people with diabetes cooking & storage:
- Use EVOO & avocado oil for salads, dips & low-temperature cooking: Doing so preserves beneficial polyphenols and keeps MUFA intake high.
- Use refined canola or high-oleic sunflower for higher-temperature cooking: they offer stability and a neutral taste while lowering saturated fat intake.
- Avoid frequent reuse of frying oil: Repeated heating creates oxidation products that may worsen inflammation and metabolic function.
- Balance omega-6 with omega-3: If you can consume seed oils high in linoleic acid. Ensure adequate omega-3 intake (fish, flax, walnuts) to support an anti-inflammatory fatty acid balance.
- Store oils correctly: Keep oils in dark, cool places and use them within the recommended period to avoid rancidity, which reduces antioxidant content and increases harmful oxidation products.
Final Recommendation Table:
| Use case/ Goal | Best choice | Acceptable | Use sparingly/ avoid |
| Daily dressing/ low-heat cooking | Extra virgin olive oil, avocado oil | Canola (cold-pressed) | Coconut oil |
| High-heat frying | Refined canola, refined high-oleic sunflower | Refined avocado oil | EVOO (not ideal for very high heat) |
| Improving insulin sensitivity | EVOO, canola, avocado | High-oleic sunflower | Coconut oil (limit) |
| Heart disease risk reduction | EVOO, canola, avocado | High- oleic sunflower | Coconut oil (limit) |
| Budget/ practical | Canola (refined) | High-oleic sunflower | Coconut oil (for flavour only) |
Disclaimer: The content on this website is for general informational and educational purposes only. It is not intended to provide medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional, doctor, or dietitian before making any changes to your diet, exercise routine, or lifestyle. Reliance on any information provided on this site is solely at your own risk.

Comments are closed.